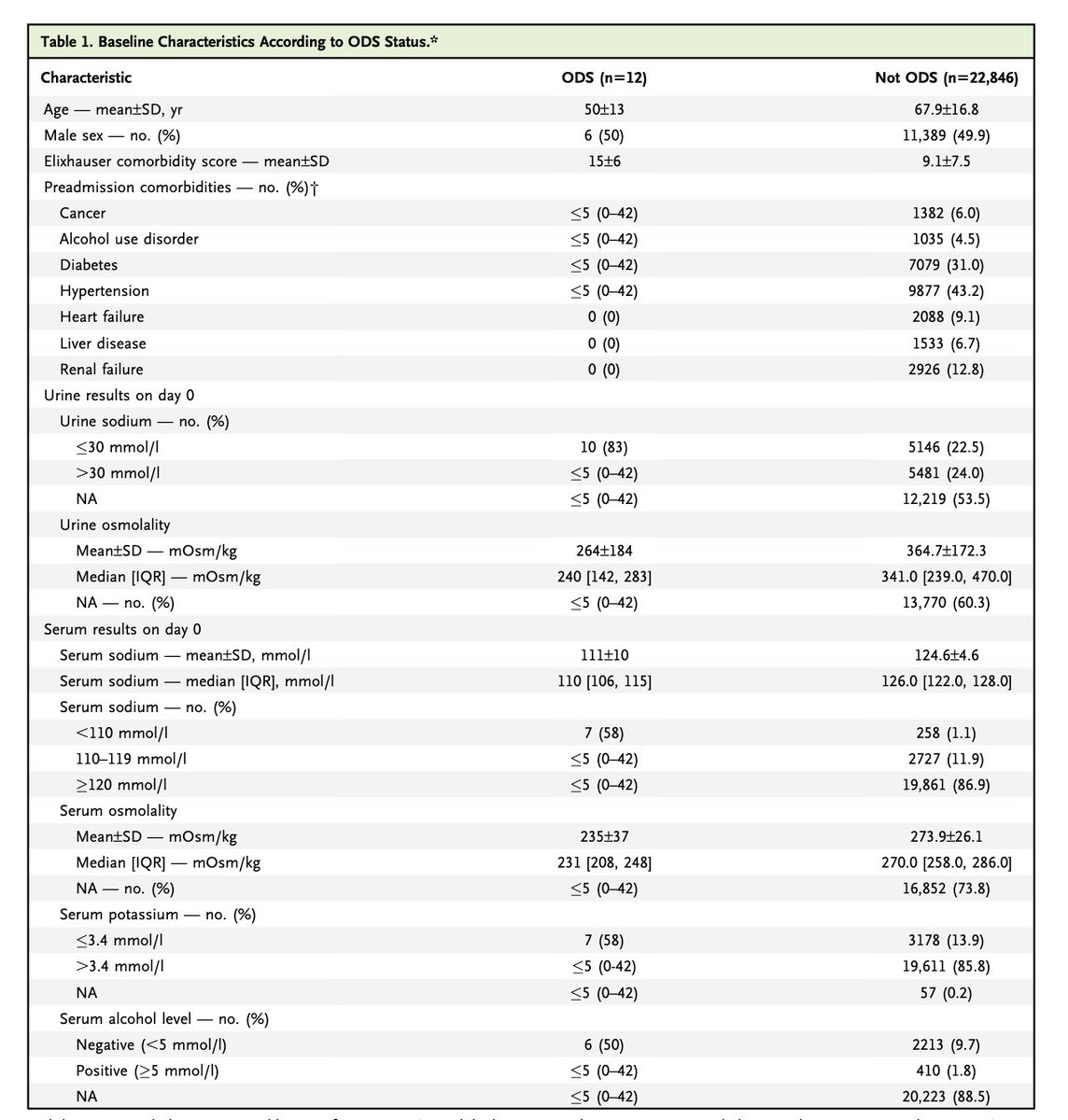
When we published our study <evidence.nejm.org/doi/10.1056/EV…> of ODS and hyponatremia we were pummeled for including people at low risk of ODS because we included Na levels between 120 and 130. They said it is well known "that ODS is incredibly rare/non-existent at those levels." 1/4
Of course one of the reasons it was thought to be incredibly rare was that no one looked for CPM in patients with Na from 120-130. We found a fair number (≤5 of 12). 2/4
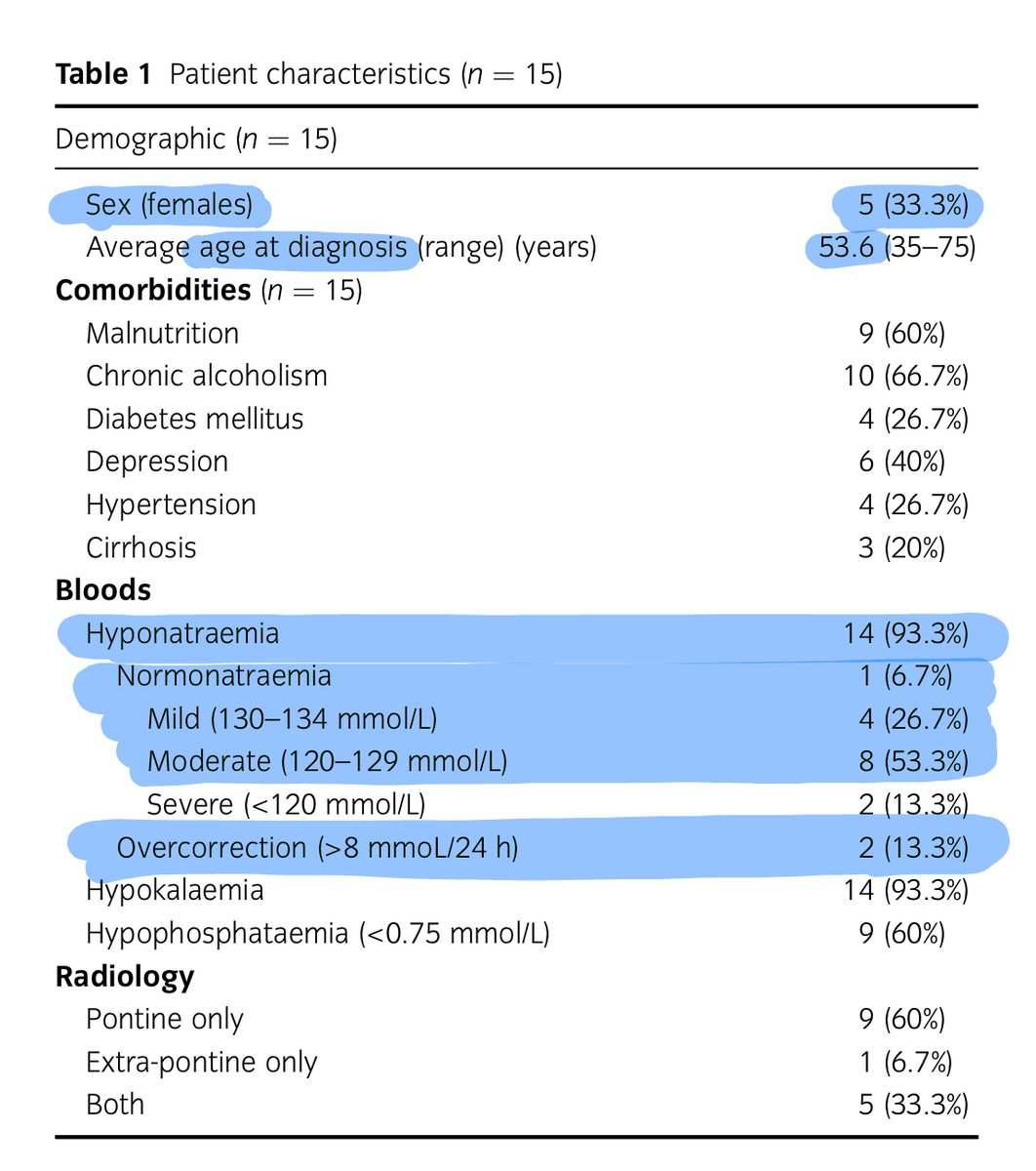
Our findings are replicated in a study from Australia. The authors took a different approach to investigating ODS. Instead of starting w/ hyponatremia and working forward to ODS, they started with a dx of ODS and worked backwards ncbi.nlm.nih.gov/pubmed/35717664 3/4
And take a look at how many of the sodiums were above 120 13 out of 15 cases Also note that only 2 patients had rapid correction of sodium😳 Malnutrition, hypokalemia, and alcohol continue to represent as they do in every study. 4/4

@kidney_boy Have we ever looked at stratifying by degree of hypo osmolality? We use Na as proxy for it, but have we looked at if the actual Osm number better reflects the risk of ODS (since it’s even in the name)?
@kidney_boy @hswapnil This goes against everything we were taught: don’t worry about rate of correction when Na>120.

@kidney_boy Eesh thank you. Seen it in ETOH +


@kidney_boy This isn’t nightmare fuel at all…

@kidney_boy @PulmCrit Thank you, very interesting. Practically speaking, which is the best approach with regard to Hyponatriemia and Hypokaliemia? Shall we correct only potassium first, even if mild, and then check sodium? 👉🏻Which potassium level shall we target ? 👉🏻 Which cristalloid to correct K+?

@kidney_boy @kidney_boy This is interesting and also consistent with findings from another paper that described >40 ODS cases and reported that the lowest average serum sodium was 131 and 75% of patients had lowest serum sodium at or above 121. pubmed.ncbi.nlm.nih.gov/34484930/
